
{kind=link}
For the past almost three years, I have written several comprehensive scientific articles demonstrating that wearing face masks won’t prevent viral diseases. In spite of the obvious facts presented by myself and other journalists, as well as numerous doctors and scientists, government officials and corporate media pundits continued to drone on about how great masks are.
Last month, the Biden administration announced that on May 11, 2023, COVID-19 national and public health emergency declarations that were put in place under former President Donald Trump in early 2020 will end. Could the reason for this be that the lies and propaganda that permeate the COVID narrative have become so blatantly obvious? It would seem so because former die-hard supporters of COVID restrictions like masks and so-called COVID vaccines have started to change their tune. They are starting to question what’s really going on. And the mainstream press is reporting it.
Example: Washington Post columnist Leana Wen MD, who is also a medical news analyst for CNN and a graduate of the World Economic Forum’s Young Global Leaders programme, was a staunch advocate of mandating masks. In February 2022, National Review reported that Wen advocated that people wear triple-ply masks even when outdoors. And that kids in school wear them. She then did a180 and now advocates that wearing masks should be up to the individual. She also stated that “masking has harmed our son’s language development” as reported in this video and in this article.
Example: Last January, Fox News reported that in her Washington Post column, Wen “admitted…that the medical community is overcounting the amount of COVID deaths and hospitalizations.” Actually, that’s an understatement: the deaths are grossly inflated. Since 2020, the CDC (Centers for Disease Control and Prevention) has reported on its website (see comorbidities and other conditions) that only over 5% of all COVID-19 deaths were due to it alone. The other 95% of COVID deaths had multiple comorbidities. In other words, they died of something else. COVID apologists try to explain away this fact by claiming that critics are misinterpreting and misrepresenting the data. But at a press conference in 2020, Dr. Ngozi Ezike, director of Illinois’ Department of Public Health succinctly states:
“I just want to be clear in terms of the definition of people dying of COVID: technically, even if you died of a clear alternate cause, but you had COVID at the same time, it’s still listed as a COVID death. Everyone who is listed as a COVID death, doesn’t mean that was the cause of the death, but they had COVID at the time of death.”
Example: On his show, Jimmy Dore presented a compilation of newscasters and government officials on TV and, in their own words, falsely claiming that the COVID shots would prevent people from getting COVID-19 and infecting others, but that Biden, Fauci and other notables all got COVID anyway. Former White House Coronavirus Response Coordinator under Donald Trump, Deborah Birx MD, best known for wearing a variety of brightly colored scarves, also admitted this when she testified before Congress back in December 2020 and in a 2022 Fox News interview said, “I knew these vaccines were not going to protect against infection. And I think we overplayed the vaccines,”
And they overplayed the masks. Reason Magazine and the New York Post, along with other mainstream publications, reported on an exhaustive January 2023 review (not to be confused with a systematic review) published by the Cochrane Library, which “found essentially no relationship between mask wearing and disease rates.” The articles, which can be read here, and here, stated in their title that “the CDC Grossly Exaggerated” the effectiveness of “mask mandates.” Both articles went on to say that the CDC “cannot be trusted as a source of public health information.”
The Cochrane review is difficult to read, but it’s not always the fault of the authors. In a February 2023 interview, lead author Dr. Tom Jefferson, MD, explained that in his previous 2020 mask review (the 2023 review is an update), his research team was “forced” to “insert unnecessary text phrases in the review” in order to get published. This and other kinds of censorship have become a common problem in scientific journals as explained in this 2020 article in Scientific American.
Dr. Jefferson also explained that Cochrane published an editorial to accompany his prior 2020 review, in his view, “to undermine our work.” He described the editorial as a call to action,“you’ve got to do something, you can’t wait for good evidence,” which is “a complete subversion of the precautionary principle,” (the precept that an action should not be taken if the consequences are uncertain and potentially dangerous). Dr Jefferson went on to say:
“…when academics and politicians started jumping up and down about masks. We call them ‘strident campaigners.” They are activists, not scientists.” Nevertheless, “…the evidence really didn’t change from 2020 to 2023. There is still no evidence that masks are effective during a pandemic.”
Levels of evidence
As explained in my previous articles, there are three kinds of scientific research: observational, experimental, and modeling (usually computational, “using computers to study something”). Observational studies, in the case of masks, are mainly epidemiological or statistical. Experimental research determines the effectiveness of masks via controlled experiments. Computer modeling is used to predict the effect that masks will have on case numbers and deaths based on their filtering capacity combined with mandates. However, only observational and experimental research count as scientific evidence. Computer modeling is highly inaccurate and does not count as scientific evidence, as illustrated by this hierarchy of scientific evidence.
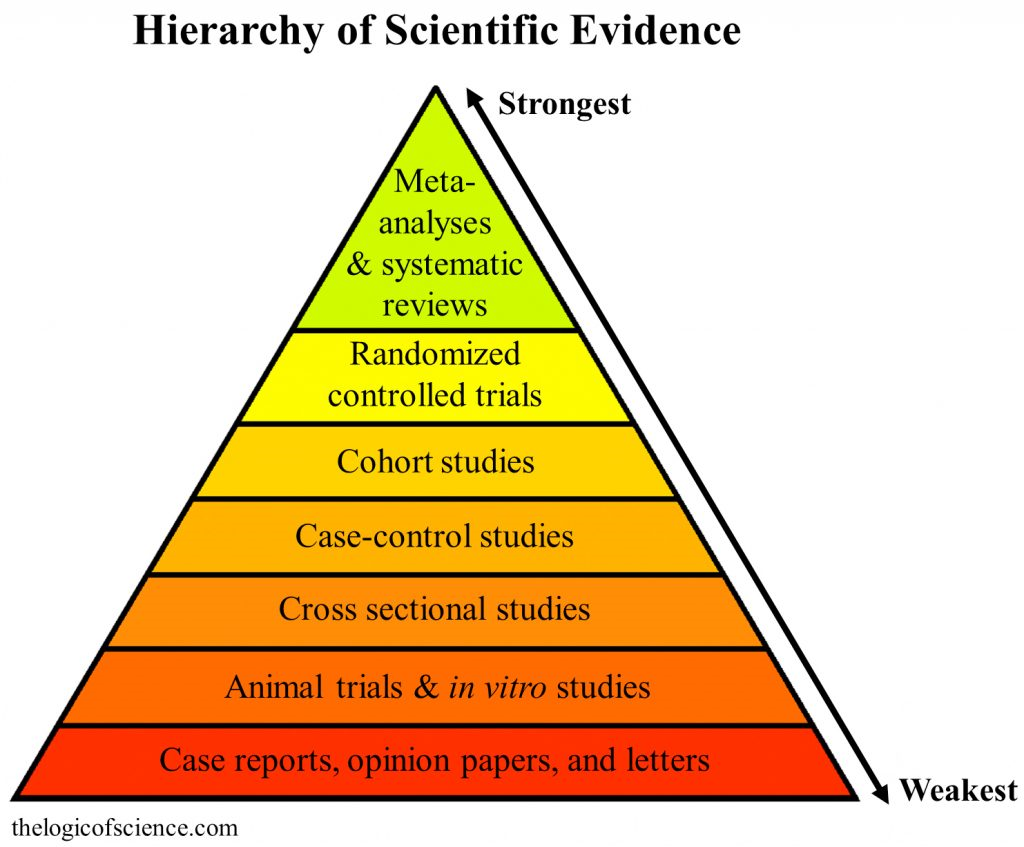
As shown in the above image, the gold standard in medical science is randomized controlled trials with verified outcomes (RCTs) combined with meta-analysis and systematic reviews, because they eliminate bias and speculation. All observational/epidemiological studies do is establish a correlation between mask wearing and COVID-19 case numbers and deaths as shown in this study. But as stated in this 2021 Harvard University article, “Observational studies can’t prove causation.”
This 2020 article in JAMA (Journal of the American Medical Association) warns that relying on weak observational studies “will hinder the goal of finding effective treatments for COVID-19—and a great many other diseases.” This is why the only studies that matter are RCTs, because they test the masks directly to see if they actually work. And every properly conducted RCT done over the past 80 years shows that masks, regardless of what kind, don’t prevent viral diseases.
Example: Canadian Family Physician. July 2020 study. 11 systematic reviews, 18 RCTs. 26,444 participants. Synthesis: “Overall, the use of masks in the community did not reduce the risk of influenza, confirmed viral respiratory infection, influenzalike illness or any clinical respiratory infection.”
Example: Emerging Infectious Diseases, peer reviewed journal published by the CDC. May 2020 study. Systematic review of 10 RCTs on the effectiveness of face masks from 1946-2018 (see Face Masks): “In pooled analysis, we found no significant reduction in influenza transmission with the use of face masks.”
Example: Annals of Internal Medicine. 2020 study conducted in Denmark. First RCT to determine if masks are effective against SARS-CoV-2, the COVID-19 virus. JAMA, the Lancet, and the New England Journal of Medicine wouldn’t publish it. The RCT involved over 6,000 Danes and found what all other RCTs found:
Discussion: “Our results suggest that the recommendation to wear a surgical mask when outside the home among others did not reduce, at conventional levels of statistical significance, the incidence of SARS-CoV-2 infection in mask wearers in a setting where social distancing and other public health measures were in effect.”
Another problem with masks is that they can severely damage the physical and mental health of adults and children. A massive comprehensive review of the many studies conducted on the health and well-being of people wearing masks was published in the International Journal of Environmental Research and Public Health in April 2021. It clearly demonstrates that mask wearing is in no way shape or form a small thing to ask of people.
Obstructing the nose and mouth with a mask causes oxygen deprivation, which increases CO2 levels in the blood, causing hypoxia, hypercapnia, headaches, confusion, physical and mental exhaustion, which the authors call MIES (Mask-induced Exhaustion Syndrome), cancer due to lower oxygen levels along with toxic substances in the masks, facial lesions, damage to teeth and gums, heart attacks, strokes, and psychological deterioration. Masks are also a breeding ground for all sorts of pathogenic microbes that “can cause clinically relevant fungal, bacterial or viral infections.”The authors emphatically state that “…mask-induced adverse changes are relatively minor at first glance, but repeated exposure over longer periods…have measurably harmful effects not only on healthy people, but also on sick people…”
A fly in the ointment?
In 2021, the peer-reviewed journal Science published a huge mask study conducted in Bangladesh that supposedly involved some 340,000 people. This randomized trial only evaluated cloth and surgical masks. N95 masks, also known as respirators, were not included. The study found no benefit in wearing cloth masks, but found an 11% decrease in symptoms associated with COVID-19 in the groups that wore surgical masks. However, the study was deeply flawed as pointed out in a 2021 paper by Dr. Denis Rancourt, PhD, a 2022 review published in ResearchGate, and in the Cochran Review led by Dr. Tom Jefferson mentioned previously.
Most importantly, the Bangladesh study was not an RCT of 340,000 people as hyped in the media. It was a “cluster randomized trial” of 300 treatment villages where there was a mask wearing intervention campaign and of 300 villages where there wasn’t. 340,000 is the total population of all the villages combined, not of how many people individually participated in the study or of how properly and consistently anyone wore masks, which there would be no way to know. Also, cluster randomized trials are “more prone to biases,” which individual RCTs are designed to eliminate, and can give a different result than individual RCTs. For example, a 2005 Cochrane review of hip protectors. “The cluster trials showed large positive effect whereas individually randomized trials did not show any clear benefit.”
Flawed logic
In July 2020, Professor Denis Rancourt, who has written scientific papers demonstrating that masks are ineffective against viral pathogens, debated Professor David Kyle Johnson who wrote scathing critiques of Rancourt’s work. While both are PhDs, Rancourt’s is in physics. He’s an actual scientist who has been published numerous times in the scientific literature. Johnson’s PhD is in philosophy. He specializes in and teaches logic and supposedly specializes in debunking pseudoscience. But judging from the debate, Johnson certainly doesn’t practice logic as far as I’m concerned. He acted like an angry, petulant, spoiled child and even threw a temper tantrum.
Johnson labeled Rancourt a conspiracy theorist and a pseudoscientist, which is the ad hominem fallacy, invalidating what is being said by attacking someone’s character or reputation. Johnson also misrepresented Rancourt’s position on COVID-19 and accused him of saying things that he didn’t say, an example of the straw man fallacy, creating “a dishonest, distorted, or otherwise inaccurate version of a person’s original argument.”
Johnson’s whole schtick was that masks can reduce the amount of infectious viral particles contained in droplets and aerosols in the air, which will reduce COVID-19 infection. He compared the filtration efficiency of masks with traffic laws against speeding, reducing accidents. This is a false equivalence fallacy, claiming two entirely different things are the same because they share similar characteristics.
Johnson’s arguments were based on inferior observational studies, computer modeling, which isn’t scientific evidence, and on mechanistic studies, which determine filtration efficiency. As explained in this EPA report and demonstrated in this 2008 HSA study in the U.K., these, and all other filtration efficiency studies show that huge amounts of infectious viral particles will always go around and through any kind of mask.
Johnson acknowledges that forcing people to wear masks won’t eliminate all infectious particles that are in the air and that they can go through masks. That’s why his arguments are fallacious. The scientific literature clearly shows that most respiratory infections are caused by “small particle aerosols,” rather than large droplets and can remain in the air indefinitely as reported in the Lancet. And as estimated by Cambridge University press, 100 COVID-19 virus particles would be enough to make a human sick. But as reported in Science Daily, even “One Virus Particle Is Enough To Cause Infectious Disease.” In reality, you will be breathing in thousands of infectious virus particles in buildings regardless of what you have on your face.
Johnson also incorrectly asserted that most large droplets existing in the mouth of an infected person wearing a mask won’t have a chance to evaporate or aerosolize into smaller microscopic particles that could possibly escape from the mask. But as reported in the International Journal of Environmental Research and Public Health review cited earlier, mask wearers exhale more fine microscopic aerosol particles than non-mask wearers, which increases the risk of infection for everyone.
Bottom line: it doesn’t matter how many droplets and aerosol particles masks filter out because MASKS DON’T WORK. It doesn’t matter what kind of mask you’re wearing because MASKS DON’T WORK. It doesn’t matter whether or not you wear your mask properly because MASKS DON’T WORK. It doesn’t matter how many comply or don’t comply with mask rules because MASKS DON’T WORK. None of these things matter because MASKS DON’T WORK.
Closing thoughts
People who buy into the mask lie think they are following the science when they are really following authoritarian orders. A consensus is defined as: “An opinion or position reached by a group as a whole.” But before we trust a scientific consensus on something like COVID-19, we need to ask the following: Is it an informed consensus? Or is it an ignorant, captured, corrupt consensus? Massive corruption in medical science is a reality as explained here and here. So, if a majority of doctors, scientists, and politicians have not studied a topic like masks, or if they have sold their souls to the highest bidder in exchange for wealth, power, and status instead of valuing truth and making the world a better place, we need not listen to them.
Everything comes with a price tag. There is no free lunch. There are positives and negatives, pros and cons, to whatever path we choose to follow. In a free society, that price will be a small class of criminals who operate outside the law. But it’s far lower than the price we are paying for a criminal government that operates within the law. So, don’t blindly believe what corrupt corporate stooges in medicine, government, and the media are telling you. Don’t allow yourselves to be bossed around by a bunch of idiots who don’t know their butt hole from a gopher hole. Doubt and question everything. A mind is a terrible thing to waste and freedom is too precious a gift to throw away.
Source of image: Facebook
izzy
- Edit
Democracy can be a dangerous thing if the population is misinformed and functionally ignorant.
Which may be the default condition in any event. Add in some manufactured fear, and it all goes off the rails fast. This “pandemic” has pulled the curtain back on a foundational American myth.
Tanner Kingston
- Edit
In the past, I’ve done confined space entry, was trained for biological war by the US military, was an EMT and then Wildland Firefighter; I’ve worked with masks of all types to save my life and got to know a fair bit as a SPOC for safety in my platoon.
Everybody I know that has used masks professionally, nurses, doctors, emergency responders, military, et al., has unequivocally stated their position against masks as a barrier of protection against SARS-COV2. I’ve read and listened to SMEs since 2020 mostly come out against this practice and yet, few listened.
When I see people wearing masks in the community today, I become sad. I see a mentally/emotionally/spiritually sick person who lives in constant fear and, given the reactions over the last three years, also as a threat to my safety and well-being.
Pompy Ciepła
- Edit
I always learn so much from your posts. This one was particularly insightful and well-written.
GlucoSlim
- Edit
For the past few days I’ve been an avid follower of this awesome site, they have brilliant content for fans. The site owner excels at captivating readers. I’m thrilled and hope they keep up their magnificent work.
NeuroTest official website
- Edit
Wonderful web site Lots of useful info here Im sending it to a few friends ans additionally sharing in delicious And obviously thanks to your effort
alevemante
- Edit
Ive read several just right stuff here Certainly price bookmarking for revisiting I wonder how a lot effort you place to create this kind of great informative website
myflixer
- Edit
Your blog is a breath of fresh air in the often mundane world of online content. Your unique perspective and engaging writing style never fail to leave a lasting impression. Thank you for sharing your insights with us.
Techno rozen
- Edit
Techno rozen I appreciate you sharing this blog post. Thanks Again. Cool.
BaddieHub
- Edit
BaddieHub very informative articles or reviews at this time.
Simplywall
- Edit
Simplywall This is my first time pay a quick visit at here and i am really happy to read everthing at one place
Free URL Shortener
- Edit
Hi, I’m Jack. Your blog is a treasure trove of valuable insights, and I’ve made it a point to visit daily. Kudos on creating such an amazing resource!
Webpanda
- Edit
This is exactly the kind of content I’ve been searching for. Thanks!
Danial Waide
- Edit
The breadth of The knowledge is amazing. Thanks for sharing The insights with us.
Sherie Linnemann
- Edit
Discovering The Writing has been a game-changer for me. The contributions are invaluable.
how much does auto glass cost
- Edit
Always excited to see The posts, like waiting for a message from a crush. Another excellent read!
Reidsville Auto Glass Replacement
- Edit
Every word you write sparkles with insight, like stars in my night sky. Can’t wait to navigate more skies together.
account activity: 2 minutes ago
- Edit
The words are like brush strokes on a canvas, painting ideas in my mind.
selected
- Edit
What a refreshing take on this subject. I completely agree with The points!
Mobile auto glass Greensboro NC
- Edit
Unique viewpoints, because who needs echo chambers?
27395 auto glass
- Edit
Thank you for the hard work you put into this post. It’s much appreciated!
WIndshield replacement Hickory,nc
- Edit
Always excited for The posts, because who else is going to make me feel this inadequately informed?
Auto Glass Shop Near Huntersville
- Edit
A breath of fresh air, or what I needed after being suffocated by mediocrity.
nooodle magazine
- Edit
Noodlemagazine Great information shared.. really enjoyed reading this post thank you author for sharing this post .. appreciated
noodlemagine
- Edit
Noodlemagazine I’m often to blogging and i really appreciate your content. The article has actually peaks my interest. I’m going to bookmark your web site and maintain checking for brand spanking new information.
Ty Gerrero
- Edit
The Writing has become a go-to resource for me. The effort you put into The posts is truly appreciated.
Noodlemagazine
- Edit
Noodlemagazine Since the admin is so committed, it’s only a matter of time before this site becomes known for its quality material.
car call adas
- Edit
The insights have added a lot of value to my understanding of the state of the country. Thanks for sharing.
adas car cal
- Edit
This was a great read—thought-provoking and informative about the state of the country. Thank you!